
This article has been temporarily removed. We apologize for the inconvenience. Find more information about circumcision and HIV here: http://www.thewholenetwork.org/research-circumcision.html#myths
|
This article has been temporarily removed. We apologize for the inconvenience. Find more information about circumcision and HIV here: http://www.thewholenetwork.org/research-circumcision.html#myths
 "Multiple logistic regressions were constructed separately to evaluate the role of circumcision in the acquisition of HIV and STI. Conclusions: [circumcision] is not associated with HIV or STI prevention in this U. S. military population."
Prevalence of male circumcision and its association with HIV and sexually transmitted infections in a U.S. navy population Thomas AG, Bakhireva LN, Brodine SK, Shaffer RA; International Conference on AIDS (15th : 2004 : Bangkok, Thailand). Int Conf AIDS. 2004 Jul 11-16; 15: abstract no. TuPeC4861. Naval Health Research Center, DHAPP, San Diego, CA, United States Background: Lack of male circumcision has been found to be a risk factor for HIV and sexually transmitted infection (STI) in several studies performed in developing countries. However, the few studies conducted in developed nations have yielded inconsistent results. Policy regarding circumcision of male infants as a prevention measure against HIV/STI remains a controversial topic. This study describes the prevalence of circumcision and its association with HIV and STI in a U. S. military population. Methods: This is a case-control study of male HIV infected U. S. military personnel (n= 232) recruited from 7 military medical centers and male U. S. Navy controls (n=516) from a general aircraft carrier population. Cases and controls completed similar self-administered HIV behavioral risk surveys. Case circumcision status was abstracted from medical charts while control status was reported on the survey. Cases and controls were frequency matched on age. Multiple logistic regressions were constructed separately to evaluate the role of circumcision in the acquisition of HIV and STI. Results: The proportion of circumcised men did not significantly differ between cases (84.9%) and controls (81.8%). Prevalence of circumcision among men born in the U. S. was higher (85.0%) than those born elsewhere (58.1%). After adjustment for demographic and behavioral risk factors lack of circumcision was not found to be a risk factor for HIV (OR = 0.9; 95% CI: 0.51, 1.7) or STI (OR = 1.08; 95% CI 0.52, 2.26). The odds of HIV infection were 2.6 higher for irregular condom users, 5 times as high for those reporting STI, 6.2 times higher for those reporting anal sex, 2.8-3.2 times higher for those with 2-7+ partners, nearly 3 times higher for Blacks, and 3.5 times as high for men who were single or divorced/separated. Conclusions: Although there may be other medical or cultural reasons for male circumcision, it is not associated with HIV or STI prevention in this U. S. military population. Read other HIV articles: New Study: Australia Rejects Circumcision as a Preventative for HIV Where Circumcision Does Not Prevent HIV  "Circumcision of infants or other minors has no place among HIV control measures in the Australian and New Zealand context; proposals such as these should be rejected."
Below is a recent study, published on October 4, 2011, by the Australian and New Zealand Journal of Public Health. You can find the original paper here. Objective: To conduct a critical review of recent proposals that widespread circumcision of male infants be introduced in Australia as a means of combating heterosexually transmitted HIV infection. Approach: These arguments are evaluated in terms of their logic, coherence and fidelity to the principles of evidence-based medicine; the extent to which they take account of the evidence for circumcision having a protective effect against HIV and the practicality of circumcision as an HIV control strategy; the extent of its applicability to the specifics of Australia's HIV epidemic; the benefits, harms and risks of circumcision; and the associated human rights, bioethical and legal issues. Conclusion: Our conclusion is that such proposals ignore doubts about the robustness of the evidence from the African random-controlled trials as to the protective effect of circumcision and the practical value of circumcision as a means of HIV control; misrepresent the nature of Australia's HIV epidemic and exaggerate the relevance of the African random-controlled trials findings to it; underestimate the risks and harm of circumcision; and ignore questions of medical ethics and human rights. The notion of circumcision as a ‘surgical vaccine’ is criticised as polemical and unscientific. Implications: Circumcision of infants or other minors has no place among HIV control measures in the Australian and New Zealand context; proposals such as these should be rejected. Australian medical authorities have discouraged routine circumcision of male infants since 1971, when the Australian Paediatric Association issued a short statement that the procedure should not be performed.1 Although this position was reaffirmed in subsequent years (1983, 1996, 2002)2 it was increasingly challenged in the late 1990s, when the medical literature began to feature ‘new evidence’ about the protective effect of circumcision against various diseases, particularly STIs. The debate intensified in 2006, after three randomised clinical trials in Africa that appeared to show circumcision could reduce a male's risk of acquiring HIV during unprotected sexual intercourse with an infected female partner by a significant degree, commonly reported as 60%, but estimated by the Cochrane Review as between 38% and 66%.3 Debate further intensified when the World Health Organization endorsed, and funding bodies provided the money for, large-scale circumcision programs in resource-poor African countries with high levels of heterosexually transmitted HIV. The question Australian public health authorities then faced was whether this evidence and advice was relevant to HIV prevention in developed countries. Answering in the affirmative have been voices from Anglophone countries with past histories of routine circumcision, who have interpreted the African evidence as a vindication of past practice. Answering with a cautious negative was the Royal Australasian College of Physicians, particularly the task force it established in 2007 to review the circumcision policy statement. In Australia the pro-circumcision argument is represented by a group associated with Professor Brian Morris, a longstanding believer in circumcision as a public health measure4 and a vehement critic of the RACP's position.5 In an editorial published in the Medical Journal of Australia he and two colleagues (Professors Cooper and Wodak, both prominent figures in the HIV policy community) presented the case for “boosting infant male circumcision in the face of rising heterosexual transmission of HIV.”6 Their intervention attracted much media attention, and so much criticism that the journal published eight letters in reply.7 The replies covered many of the grounds for dissenting from the proposition that Australia's HIV problem demanded circumcision of infant males, including relevance, effectiveness, the risk of injury, harm and complications, and whether the proposal was in line with established principles of evidence-based medicine, medical ethics and human rights. Appreciating that the target of the editorial was the RACP position, the chairman of the task force that had just finalised the new policy statement defended its conclusion that circumcision should still not be recommended. A surprising omission from the replies was that none asked why the editorial had devoted so little effort to establishing the conditions that would have to be met in order to make widespread neonatal circumcision as an HIV control strategy appropriate in the Australian context. To prove the argument, it would have had to demonstrate that:
Despite the hostile reaction to the proposal, the issue is not likely to die down in the near future, particularly as other medical authorities in Canada and the US are considering the issue and are expected to issue their own policies later this year. It is therefore appropriate to subject the circumcision prescription to a more detailed analysis. In this paper it is argued that the proposal is fatally flawed because:
The claim that circumcision prevents heterosexual HIV transmission from women to men is based on three non-double-blinded, non-placebo-controlled Random-controlled trials in Africa, in which 5,400 men were circumcised. After 20 months, 64 of the men in the circumcised experimental groups had HIV, compared to 137 in the non-circumcised control groups. Six hundred and seventy-three men were lost to follow-up, their HIV status unknown.8–10 Cooper et al. take the claimed results of these trials at face value and ignore serious doubts about their validity and applicability. As several critiques have pointed out,11–15 they fell far short of the so-called ‘gold standard’, vitiated by several forms of bias, especially selection bias, since only men interested in a free circumcision were eligible. All participants were to be circumcised, some immediately, the remainder at the conclusion of the trial. Since participants assigned to immediate circumcision were aware that they had received the treatment rather than being placed in the control group, it was impossible to blind either the researchers or the subjects. Without sham surgery there could be no placebo. The trials also suffered from expectation bias (both researcher and participant), lead-time bias, attrition bias, and premature termination.16 All these weaknesses favoured the results the investigators expected. Perhaps the most crucial flaw in these three studies is that the researchers assumed that all the men who became HIV positive during the course of the trials were infected through sexual contact. When the study results are examined closely, there is evidence that as many as half the infections could have been acquired non-sexually. In the South African trial, for example, 23 men became infected even though they had either no sexual contact or always used a condom.17 If a significant number of the men who became infected in this experiment did so through non-sexual contact, it becomes impossible to accurately estimate the protective effect of circumcision on sexual transmission of HIV. A further problem with the random-controlled trials is that we do not know whether their results can be replicated in other high-prevalence sites outside a research setting, with their resources, expertise and monitoring, or in general, low-prevalence sites. It will be many years before we learn whether the current African circumcision programs have succeeded in significantly reducing HIV prevalence in the general population, and African population surveys suggest that the results of the clinical trials are not likely to have external validity.18 Garenne found that in eight countries (Burkina Faso, Cote d'Ivoire, Ethiopia, Ghana, Niger, Rwanda, Tanzania and Zimbabwe) there was no significant difference in HIV seroprevalence between circumcised and uncircumcised men; in two countries (Kenya and Uganda) HIV seroprevalance was higher among uncircumcised men; and in three countries (Cameroon, Lesotho and Malawi) HIV seroprevalence was significantly higher among circumcised men. In Lesotho the difference was striking: HIV seroprevalence was 22.8% among the circumcised, but only 15.2% among the uncircumcised.19 In South Africa, where a third of the population is circumcised and HIV prevalence is among the highest on record, both Garenne and Connolly et al. found no difference in HIV status between circumcised and uncircumcised samples.20 As Garenne comments, “large-scale demographic surveys, as well as routine seroprevalence surveys among pregnant women, do not show any consistent population impact of male circumcision on either HIV prevalence or HIV incidence.”21 Both the United States and Indonesia, with predominantly circumcised male populations, have a significantly higher incidence of HIV than Australia, Canada, Britain and New Zealand, where circumcision is in decline or extremely rare.22 In the United States, African-Americans exhibit both the highest rate of circumcision and the highest rate of heterosexually-transmitted HIV.23,24 Such is the faith in Western health advice, however, that in Swazliland, with an HIV prevalence of 22% among circumcised men but only 20% among the uncircumcised, the government has still announced a particularly ambitious circumcision program.25 Another objection to regarding circumcision as effective prophylaxis against HIV is that there is no convincing biological explanation of its protective effect.26 Circumcision advocates have speculated that the interior mucosa of the prepuce is thinner and more prone to tearing. While a thinner epithelial layer of genital tissue may be associated with increased internal transfer of HIV,27 the mucosa of the inner and outer prepuce have been shown to be of the same thickness in some studies28 but not in others.27 It is also suggested that HIV is more likely to be transmitted through the foreskin because it has a high concentration of Langerhans cells, believed to be the entry point for the virus. Actually, Langerhans cells are quite efficient in repelling HIV, which may explain the low transmission rate of HIV – only about one per 1,000 unprotected coital acts.29 The inner foreskin secretes langerin, which is effective in killing numerous pathogens.30 Langerhans cells may also provide protection against other STIs, which may explain why circumcised men are at greater risk of infection with some STIs, such as urethritis.31 Until we understand how circumcision works biologically, we cannot be certain whether the observed reduction in risk of infection in the random-controlled trials is the result of changed anatomy resulting from surgery, changed behaviour resulting from counseling and provision of condoms, or the various forms of bias built into the studies. Circumcision advocates have portrayed the sub-preputial space as a harbour for sexually transmitted viruses.32 Against this, however, meta-analyses assessing susceptibility to genital infections with herpes simplex virus and human papilloma virus have not shown any meaningful association with circumcision status.33,34 Unfortunately, these portrayals have appeared so often in the medical literature that many physicians and public health officials consider them factual. There is, however, no scientific proof that the foreskin is a predisposing factor for infections of this kind. The most serious objection to the circumcision proposal is that it is not applicable to our situation. Australia is not sub-Saharan Africa, where HIV is a generalised epidemic transmitted largely by heterosexual intercourse and non-sterile medical equipment.30,35 In Australia, HIV is a relatively low-prevalence disease, largely contained within the specific sub-cultures where it has always been found: mostly homosexual men (80%), plus a very small population of injecting drug users (4%).36 Although Daniel Halperin advised gay men who take the insertive role in anal intercourse to get circumcised,37 it is now firmly established that circumcision provides no protection to men who have sex with men (MSM),38–41 and there is evidence from Britain that circumcised gay men may be at greater risk.42 Whether that is generally the case, it is obvious that circumcision would have made no difference to the vast majority of Australian men who have become HIV positive over the past thirty years. Cooper et al. are not so misguided as to suggest that either gay men or injecting drug users would receive any protection from circumcision, but focus on the small incidence of heterosexual transmission. This is running at such a low level, however, that the circumcision proposal is grossly out of proportion to the problem. The surveillance authority of which Cooper himself is director expresses no alarm, and in its latest report points out: “the annual number of new HIV diagnoses has remained relatively stable at around 1000 over the past four years”; “HIV continues to be transmitted primarily through sexual contact between men”; and “of 1185 cases of (heterosexually acquired) HIV infection newly diagnosed in 2005–2009, 58% were in people from high prevalence countries or their partners”.43 The total number of newly diagnosed HIV infections in 2009 was 1,050, of which males made up 86.7%, down slightly from 87.4% in 2001. Over the same decade, the proportion of newly diagnosed infections among MSM has remained steady: 66.6% in 2001, 65.1% in 2009. The increase in the proportion of infections attributable to heterosexual contact from 21.8% in 2001 to 28.7% in 2009 is neither a dramatic rise nor cause for alarm, especially as nearly 60% of such infections occur in people with a partner either HIV-positive or in a high-risk category.44 The 1,185 cases of heterosexual transmission in the five years 2005–09 represent about 200 new diagnoses annually, but since the infection could have been acquired at any time this is not evidence of new cases or a rising trend. Because more than half of these are found in people from, or with a partner from, a high-prevalence country it is possible that many of these infections were not acquired in Australia. A more relevant measure are newly acquired infections – new infections that were definitely acquired in the previous twelve months – and here there is even less cause for alarm. In 2005–09, 82% of newly acquired infections were in MSM, 3% among injecting drug users, and 10% from heterosexual contact.45 Cooper et al. refer to a rising proportion of female-to-male transmission, but the numbers are still very small (23 men newly infected in 2009), and the rate of increase is both erratic and slow. Click to see Table 1. Characteristics of newly-acquired HIV infection 2000–2009
The proposal is also irrelevant because it targets infants rather than adults. Infants are not at risk of infection by sexual contact and will not be at risk until they become sexually active in 16–20 years time, by which time treatment and prevention options, and the virus itself, may have altered beyond recognition. Evidence-based medicine requires that recommendations for treatment or prophylaxis follow logically and directly from the evidence. Assuming the African evidence is reliable and applicable, the logical prescription is that sexually active adult men who have regular intercourse with numerous female partners and do not always use condoms should consider circumcision for themselves. One approach might be that sexual health advice targeted at this category could include circumcision as a prophylactic option among a range of sexual health offerings, as the WHO has recommended. This is not what Cooper et al. prescribe. Instead, they propose that parents be advised to circumcise their baby boys as a precaution against a risk they will not face until adulthood, and against a disease that is very rare among heterosexually active adult men anyway. Even if circumcised, they would still need to use a condom to be certain of avoiding infection, since the risk reduction indicated by the African data is only partial (38%–66%). We have no evidence on what the risk reduction in a low-prevalence country such as Australia might be, and with such a low level of heterosexual transmission it would be neither feasible nor ethical to mount random-controlled trials. If it is still necessary to wear a condom there seems little point in getting circumcised. As Perera et al. point out,49 moreover, the African trials involved sexually active adult men, not infants, and there is no hard evidence that neonatal circumcision has any protective effect against HIV. The prescription has little connection with the evidence on which it is presumed to depend and thus violates the principles of evidence-based medicine. As subsequent research has confirmed,50,51 the WHO recommendations arising from the African random-controlled trials cannot be applied to developed nations, but only to regions of high HIV prevalence, in generalised epidemics with predominantly heterosexual transmission. Medical authorities responsible for formulating policy statements on neonatal circumcision have reached the same conclusion. In a strongly-worded statement against prophylactic circumcision of minors, the Royal Dutch Medical Association comments: “That the relationship between circumcision and transmission of HIV is at the very least unclear is illustrated by the fact that the US combines a high prevalence of STDs and HIV infections with a high percentage of routine circumcisions. The Dutch situation is precisely the reverse: a low prevalence of HIV/AIDS combined with a relatively low number of circumcisions. As such, behavioural factors appear to play a far more important role than whether or not one has a foreskin.”52 The RACP reached the similar conclusion that “in low prevalence populations such as Australia and New Zealand circumcision does not provide significant protection against STIs and HIV, and is less effective than safe sex practices.”53 Cooper et al. state that “The protection conferred to heterosexual males by circumcision is similar in hyperendemic and low-prevalence settings”. This claim – crucial to their argument – is not supported by their citations, which carefully note that recommendations based on the trials pertain only to similar settings, i.e., in generalised epidemics with high HIV prevalence. That is not the kind of epidemic found in Australia. Supporters of circumcision claim other benefits of early circumcision, but such arguments are irrelevant to the question of HIV infection itself. But even these additional claims are either contested to the point of inconclusiveness or rejected as invalid or irrelevant. Perera et al. found the benefits of neonatal or childhood circumcision to be negligible and the possibility of reduced vulnerability to HIV irrelevant to children.49 If uncircumcised boys are more subject to “adverse medical conditions”, as Cooper et al. claim, we would expect this to show up in child health reviews, but the Australian Institute of Health and Welfare found no decline in child health as the incidence of circumcision in Australia has fallen, and indeed that child health has improved over the same period.54 The RACP concluded that there was no medical justification for prophylactic circumcision of minors in Australia.53 Two glaring omissions from Cooper et al's argument are discussions of the harm and risks of circumcision and the ethics of performing amputative surgery on minors. Research on the anatomy and physiology of the foreskin is primitive, but we know that it is an anatomically integral, sexually functional and psychologically significant component of the penis, loss of which may have adverse consequences on both sexual satisfaction and psychological well-being.55 The extent to which the foreskin contributes to sexual function is in dispute,56–59 but research is so inadequate that nobody can say with confidence that circumcision ‘makes no difference’. The RACP policy statement acknowledges that the foreskin is the most sensitive part of the penis and points out that since men may resent having been circumcised as infants, it may be preferable to delay the operation until a boy reaches maturity and can give informed consent.53 It might be assumed that resentment would be less if all boys were circumcised at birth, but even when they grow up among circumcised peers many men can still feel angry and mutilated, even to the point of psychological disturbance.60 Cooper et al. cite a study claiming that neonatal circumcision is “cost effective”,61 but in fact the article was a cost analysis that did not consider cost effectiveness at all. Others have concluded that since the procedure both adds to health costs and reduces the overall health of the individual it can be justified on neither economic nor medical grounds.62 Any consideration of the costs of circumcision will be woefully inadequate if it fails to factor in the value of the foreskin to the individual and the cost of surgical complications and other adverse sequelae, both physical and psychological. Complications from circumcision are another area where lack of both adequate data and benchmarks for acceptable risk make it impossible to be confident that the operation is ‘safe’. While all circumcisions result in the loss of the most sexually responsive portion of the penis, accurate estimates of the incidence and severity of complications are not available. In 2002 the RACP cited estimates ranging from an implausible 0.06% to an equally unlikely 55%, depending on definition, but regarded the likely incidence as falling somewhere between 2% and 10%, and warned that “serious complications, such as bleeding, septicaemia and meningitis may occasionally cause death”.63 Reported complication rates are heavily influenced by how a complication is defined and how the data is collected. One study that assessed all infants for bleeding found that circumcision resulted in excessive bleeding in 8.9% to 9.9% of cases.64 Many common complications may not be documented because they are considered par for the course, yet chart reviews have documented complication rates between 3.2%65 and 6.8%.66 Delayed complications such as meatal stenosis are often missed, yet the rate of meatal stenosis following circumcision ranges from 5% to 20%,67,68 while problems such as excessive tissue removal may not become evident until after puberty.69 Although practitioners claim that the Plastibell is a safer instrument than clamps, there are many reports of complications from this device, including two recent deaths.70–72 There is no evidence at all for the assertion that neonatal circumcision presents a lower incidence of complications than circumcision in adulthood. Indeed, one study (from a circumcising culture) found the incidence of complications in the neonatal period so high that it recommended leaving the procedure until later.73 In Australia, Leitch (1970) reported a complication rate of 15.5%,74 while a doctor who performed medical examinations of schoolboys reported that he was “appalled at the phallic mutilations exhibited by many of these children, some of whom have even been subjected to a subsequent ‘tidying up’ procedure after being badly mauled in infancy.”75 The risk of harm is likely to be greater if the operation is performed before the natural separation of foreskin from glans, and lower in adulthood, when the mature size of the penis and final foreskin length can be observed and taken into account. Males differ so much in these variables that one cut does not fit all.76 Unlike a newborn infant, moreover, an adult patient can be safely given both effective anaesthesia and post-operative pain relief. Circumcision advocates must consider adult circumcision perfectly safe, or they would be criticising the African circumcision programs for posing an unacceptable risk of harm to the men who enrol in them. Even if the circumcision proposal were relevant to the Australian situation, to be ethically acceptable a medical intervention must pass the five tests proposed by Beauchamp and Childress:
While we all hope that a vaccine for HIV will eventually be developed, the tendency to describe circumcision hyperbolically as a ‘surgical vaccine’ is regrettable and misleading. The comparison may appeal to scientifically naive journalists, but it has no basis in science and is irresponsible from a public health perspective, in that it may encourage high-risk behaviour.81 Circumcision provides nothing like the kind or level of protection provided by a vaccine, merely a risk reduction in one specific situation (unprotected heterosexual intercourse in a high seroprevalence setting). Circumcision advocates seem unwilling to acknowledge the difference between amputating body parts to provide limited protection against a rare disease to which the individual is unlikely to be exposed, and giving a person a needle that confers a high level of immunity to common or highly contagious diseases. The justification for vaccinating non-consenting children is first, that it does not involve the removal of a functional body part, and secondly that the diseases to which it confers immunity are common and/or highly contagious.82 Airborne diseases, such as smallpox, diphtheria, and measles were all major killers before vaccines. Because such diseases are spread by breathing, a single child can infect a whole school. Vaccination thus protects both the individual who receives the treatment and the people with whom he comes into contact. Unlike these diseases, HIV is a low-virulence, and in Australia, a rare disease that can be avoided by appropriate risk-reducing behaviour. The colourful image of circumcision as ‘surgical vaccine’ is a contradiction in terms, on a par with ‘conjectural fact’; such rhetoric has no place in scientific debate. Although this explanation has been questioned,83 it is generally accepted that the rapid spread of HIV in Africa was associated with a high level of sexual activity, involving numerous concurrent, but often transient sexual partnerships, widespread prostitution, both formal and informal, various forms of polygamy, and reluctance to practise safe sex or use condoms. It is also probable that a significant proportion of HIV infections are the result of non-sexual transmission, such as non-sterile medical procedures.84 These conditions were aggravated by poorly developed health services, the co-presence of numerous other epidemic diseases, such as malaria, tuberculosis and other STIs, and the refusal of local authorities to take action until the disease had spread through the population, provoked by the misconception that AIDS was a ‘gay disease’, confined to the decadent developed world.85 This crisis situation stands in dramatic contrast to that of a wealthy, developed nation such as Australia, where effective action was taken early on, based on respect for the autonomy and agency of those at greatest risk, and an emphasis on safe sex education, needle and syringe programs, and provision of condoms. This strategy has been strikingly successful: AIDS in Australia remains a relatively minor public health problem, largely confined to the sub-cultures where it has traditionally been found. There is no heterosexual epidemic that would justify a costly, authoritarian program of the type and scale that Cooper et al. propose. There is every reason to think that the strategy that Australia has pursued so successfully since the 1980s will continue to protect the vast majority of the population from this disease.86
 Have you heard that circumcision reduces HIV transmission? Here's an accurate breakdown of exactly why circumcision does NOT prevent HIV. Written by: Joseph4GI (read the original article here) Posted with Permission from Author There's currently a lot of hype surrounding circumcision and the transmission of HIV. The word on people's lips is that "circumcision reduces HIV transmission by 60%." The claim is based on the result of three major "studies" that were carried out in Africa, but there are a few confounding factors that bring the validity of these so-called "studies" into question. One of the greatest confounding factors in these studies is empirical evidence to the contrary; real world data from countries where circumcision is already a widespread practice and studies with contrary results. Countries in Africa Let's begin with countries in Africa, where these "studies" would be relevant. According to demographic health surveys performed in other countries in Africa, HIV transmission was prevalent in circumcised men in at least 6 different countries. I go one by one, analyzing some of the commentary in these surveys, some of which seems to be revealing of the researchers' bias. Cameroon In Cameroon, where 91% of the male population is circumcised, the ratio of circumcised men vs. intact men who contracted HIV was 4.1 vs. 1.1. (See p. 17) http://www.measuredhs.com/pubs/pdf/FR163/16chapitre16.pdf Ghana "...the vast majority of Ghanaian men (95 percent) are circumcised... There is little difference in the HIV prevalence by circumcision status..." (1.6 vs 1.4 See p. 13) http://www.measuredhs.com/pubs/pdf/FR152/13Chapter13.pdf Lesotho In Lesotho, 23% of the men are circumcised, and the ratio circumcised men vs. intact men who contracted HIV was 22.8 vs 15.2. "The relationship between male circumcision and HIV levels in Lesotho does not conform to the expected pattern of higher rates among uncircumcised men than circumcised men. The HIV rate is in fact substantially higher among circumcised men (23 percent) than among men who are not circumcised (15 percent). Moreover, the pattern of higher infection rates among circumcised men compared with uncircumcised men is virtually uniform across the various subgroups for which results are shown in thetable. This finding could be explained by the Lesotho custom to conduct male circumcision later in life, when the individuals have already been exposed to the risk of HIV infection. (Additional analysis is necessary to better understand the unexpected pattern in Table 12.9.)" (p. 13) What is disturbing here is that it seems researchers grope for a reason to dismiss these results because they are not what they are looking for; a positive result for circumcision. The above is an interesting defense of male circumcision, given the fact that the latest "studies," if they can even be called that, observed HIV trasmission in men circumcised as adults. Then again, this demographic health survey was conducted in 2004, BEFORE the newer "studies" in 2006. None the less, the unproven assertion that "circumcision is only effective in reducing the risk of HIV when done in infancy" persists in some circles. http://www.measuredhs.com/pubs/pdf/FR171/12Chapter12.pdf Malawi In Malawi, 20% of the male population is circumcised. The ratio of circumcised vs. intact men who contracted HIV was 13.2 vs 9.5. "The relationship between HIV prevalence and circumcision status is not in the expected direction. In Malawi, circumcised men have a slightly higher HIV infection rate than men who were not circumcised (13 percent compared with 10 percent). In Malawi, the majority of men are not circumcised (80 percent)(...where one would expect HIV to be the most rampant... note the "expected direction.") (p. 10) http://www.measuredhs.com/pubs/pdf/FR175/12Chapter12.pdf Rwanda According to a demographic health survey taken in 2005, the ratio of circumcised vs. intact men who contracted HIV was 3.8 vs 2.1. (See p. 10) http://www.measuredhs.com/pubs/pdf/FR183/15Chapter15.pdf Swaziland In a recent demographic health survey (2006-2007), the ratio of circumcised vs. intact men who contracted HIV was found to be 22 vs. 20. As Table 14.10 shows, the relationship between HIV prevalence and circumcision status is not in the expected direction. Circumcised men have a slightly higher HIV infection rate than men who are not circumcised (22 percent compared with 20 percent). (p. 256) http://www.measuredhs.com/pubs/pdf/FR202/FR202.pdf Here is that "expected direction" again. The majority of Swazi men are uncircumcised, and one would especially expect to see HIV prevalence here. HIV transmission was more prevalent in the circumcised men here, yet our (the US) government has decided to spend millions on a campaign to circumcise 80% of the men in Swaziland. http://joseph4gi.blogspot.com/2011/05/soka-uncobe-our-us-tax-dollars-at-work.html Other Countries Where HIV/Circumcision Rates Don't Correlate Malaysia According to Malaysian AIDS Council vice-president Datuk Zaman Khan, more than 70% of the 87,710 HIV/AIDS sufferers in the country are Muslims. In Malaysia, most, if not all Muslim men are circumcised, whereas circumcision is uncommon in the non-Muslim community. 60% of the Malaysian population is Muslim, which means that HIV is spreading in the community where most men are circumcised at an even faster rate, than in the community where most men are intact. http://www.mmail.com.my/content/39272-72-percent-aidshiv-sufferers-malaysia-are-muslims-says-council The Philippines In the Philippines, the majority of the male population is circumcised, as it is seen as an important rite of passage. In the 2010 Global AIDS report released by UNAIDS in late November, the Philippines was one of seven nations in the world which reported over 25 percent in new HIV infections between 2001 and 2009, whereas other countries have either stabilized or shown significant declines in the rate of new infections. Among all countries in Asia, only the Philippines and Bangladesh are reporting increases in HIV cases, with others either stable or decreasing. http://globalnation.inquirer.net/news/breakingnews/view/20110102-312124/Philippines-HIVAIDS-problem-worries-UN Israel Despite circumcision being near-universal, it hasn't stopped HIV transmission in Israel. http://www.haaretz.com/print-edition/opinion/failing-the-aids-test-1.249088 http://www.haaretz.com/print-edition/features/israeli-gays-shun-condoms-despite-worrying-rise-in-aids-1.249372 http://www.haaretz.com/news/has-the-aids-cocktail-worked-too-well-in-israel-1.258520 http://www.haaretz.com/print-edition/news/hiv-diagnoses-in-israel-climb-new-cases-among-gays-up-sharply-1.248651 The most obvious smoking gun: The United States of America Circumcision hasn't stopped HIV in our own country. http://data.unaids.org/pub/Report/1998/19981125_global_epidemic_report_en.pdf And, it hasn't stopped other STDs either. http://www.reuters.com/article/2009/01/13/us-infections-usa-idUSTRE50C5XV20090113?pageNumber=1&virtualBrandChannel=0 In America, the majority of the male population is circumcised, approximately 80%, while in most countries in Europe, circumcision is uncommon. Despite these facts, our country does poorly. http://www.advocatesforyouth.org/index.php?option=com_content&task=view&id=419&Itemid=177 In fact, AIDS rates in some US Cities rival hotspots in Africa. In some parts of the U.S., they're actually higher than those in sub-Saharan Africa. According to a 2010 study published in the New England Journal of Medicine, rates of HIV among adults in Washington, D.C. exceed 1 in 30; rates higher than those reported in Ethiopia, Nigeria or Rwanda. http://www.nejm.org/doi/full/10.1056/NEJMp1000069 The Washington D.C. district report on HIV and AIDS reported an increase of 22% from 2006 in 2009: "[Washington D.C.'s] rates are higher than West Africa... they're on par with Uganda and some parts of Kenya." Shannon L. Hader, HIV/AIDS Administration, Washington D.C., March 15, 2009 She once led the Federal Centers for Disease Control and Prevention's work in Zimbabwe.http://www.washingtonpost.com/wp-dyn/content/article/2009/03/14/AR2009031402176.html One would expect for there to be a lower transmission rates in the United States, and for HIV to be rampant in Europe; HIV transmission rates are in fact higher in the United States, where most men are circumcised, than in various countries in Europe, where most men are intact. It is telling that the HIV epidemic struck in our country in the 1980s, 90% of the male population was already circumcised. Somehow, we're supposed to believe that what didn't worked in our own country, or anywhere else, is going to start working miracles in Africa. Studies With Contrary Conclusions 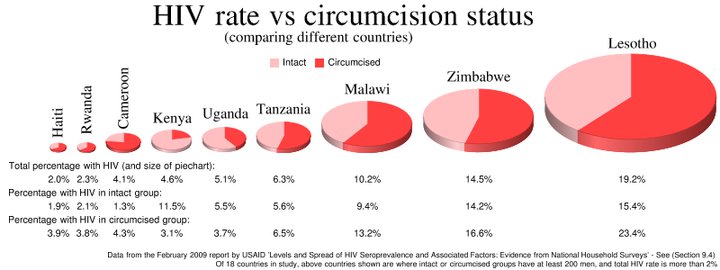 According to USAID, "there appears no clear pattern of association between male circumcision and HIV prevalence—in 8 of 18 countries with data, HIV prevalence is lower among circumcised men, while in the remaining 10 countries it is higher."
http://www.measuredhs.com/pubs/pdf/CR22/CR22.pdf "Conclusions: We find a protective effect of circumcision in only one of the eight countries for which there are nationally-representative HIV seroprevalence data. The results are important in considering the development of circumcision-focused interventions within AIDS prevention programs." http://www.iasociety.org/Default.aspx?pageId=11&abstractId=2197431 Results: ...No consistent relationship between male circumcision and HIV risk was observed in most countries. http://apha.confex.com/apha/134am/techprogram/paper_136814.htm One study which aimed at measuring male to female HIV transmission was ended early, because the results were not looking favorable. The Wawer study showed a 54% higher rate of male-to-female transmission in the group where the men had been circumcised. The figures were too small to show statistical significance, but there will be no larger scale study to find out if circumcising men increases the risk to women. Somehow that's considered unethical, yet it's considered ethical to promote male circumcision while not knowing if the risk to women is increased (by 54%?, 25%?, 80%? - who knows?) http://www.thelancet.com/journals/lancet/article/PIIS0140-6736%2809%2960998-3/fulltext The latest study in Kenya finds no association between male circumcision and lowered HIV rates: 'Using a population-based survey we examined the behaviors, beliefs, and HIV/HSV-2 serostatus of men and women in the traditionally non-circumcising community of Kisumu, Kenya prior to establishment of voluntary medical male circumcision services. A total of 749 men and 906 women participated. Circumcision status was not associated with HIV/HSV-2 infection nor increased high risk sexual behaviors. In males, preference for being or becoming circumcised was associated with inconsistent condom use and increased lifetime number of sexual partners. Preference for circumcision was increased with understanding that circumcised men are less likely to become infected with HIV.' Conclusion A few select studies show a prevalence of HIV transmission in uncircumcised men, but real world empirical data shows that circumcision hasn't stopped HIV in countries where there is already a prevalence of the practice of circumcision, nevermind the United States. Yet, for whatever reason, leaders at the WHO continue to endorse it as HIV prevention policy and millions are being spent on so-called "mass circumcision campaigns," even in countries where HIV transmission was shown to be prevalent among the circumcised. As if the waste of money weren't bad enough, reports are showing that these "mass circumcision" campaigns are actually proving to be disastrous, as they are confusing African citizens, and many now believe to be fully protected by circumcision. http://joseph4gi.blogspot.com/2011/05/male-circumcision-and-hiv-in-africa.html Something must be done to alert our world leaders. Millions of precious funds are being used to promote a worthless surgical procedure that leaves men with permanently altered organs, and they are no better protected. The false security that the promotion of circumcision creates is actually helping to facilitate the spread of HIV. Funds are already scarce, and they could be better spent promoting cheaper, less invasive modes of prevention that have actually been proven to be conclusively effective, such as condoms and education. In light of the real-world evidence, promoting a worthless surgical procedure is an impertinent disservice in the fight against HIV/AIDS and governments need to be told to stop. Africans deserve better. |

© 2010-2023
The WHOLE Network All rights reserved. Do not copy/paste articles or photos without author's express written permission. Contact guest authors through theWHOLEnetwork@gmail.com These articles are merely the opinions of the authors and are not in any way, shape, or form a substitute or replacement for proper medical treatment, and do not constitute medical advice. Recent Articles:Categories
All
Archives
May 2017
 |

 RSS Feed
RSS Feed
